Cough
PKGhatak, MD
Cough is a protective action, either voluntary or reflex, to clear the airway of secretion.
The pharynx is a Greek word meaning the throat. The throat is a hollow muscular structure, stretches from the base of the skull to the beginning of the larynx in front and the esophagus behind. Epiglottis is a cartilaginous structure guarding the openings of the larynx and esophagus. The upper posterior part of the pharynx is the nasopharynx where nasal passages open. The middle part is the oropharynx, an extension of the oral cavity and the lower part is the laryngeal pharynx.
The sensation from the nasopharynx is carried by the maxillary branch of the trigeminal nerve (cranial nerve 5). The oropharynx is innervated by the sensory division of the glossopharyngeal nerve. The larynx, vocal cords and nasopharynx are innervated by the sensory fibers of the Vagus nerve –the internal division of the superior laryngeal nerve. A sensory branch of the Vagus also supplies a portion of the external auditory canal and Eustachian tube. Branches from these nerves form a tangle of nerves called the Pharyngeal plexus. The trachea and bronchus down to the respiratory bronchioles are innervated by the recurrent laryngeal nerve of the vagus. These nerves carry sensation to the brain. But the cough center in the brain is not a localized center.
The motor impulse to the muscles involved in the cough reflex is supplied by several nerves. The main muscle is the diaphragm: The phrenic nerve innervates the diaphragm. The intrinsic muscles of the Pharynx are supplied by the recurrent laryngeal nerve, and only the stylopharyngeus muscle is innervated by the motor fibers of the glossopharyngeal nerve. The external intercostal muscles, anterior abdominal muscles, are innervated by the intercostal nerves of the thoracic segments of the spinal motor nerves of the abdomen.
Mechanism of cough.
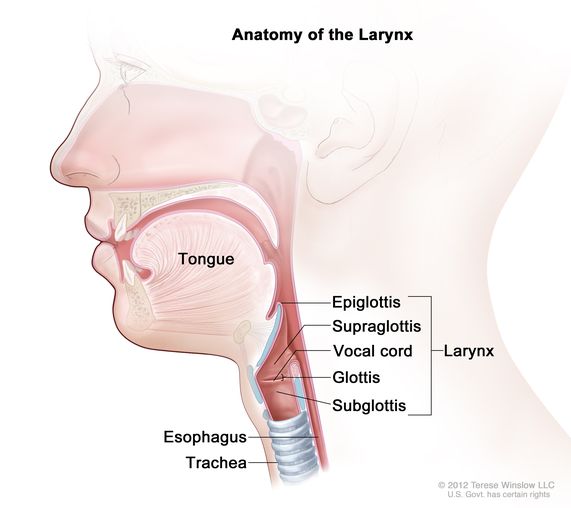
The initial action is the closure of the glottis (the vocal cords and the space between them), the epiglottis closes the opening to the larynx. The next act is a forceful contraction of all muscles, resulting in positive pressure in the thoracic cavity. The trachea and bronchus become shorter and narrower. The last act is the sudden relaxation of the vocal cord and throat. That results in a sudden gush of air expelled from the airways carrying all irritants captured in the bronchial secretion.

Though coughing and sneezing are triggered simultaneously with some common noxious stimuli, these two reflexes are different. A person can cough in sleep or under light anesthesia. On the other hand, a person who has to be awake to sneeze at the same time cannot sneeze voluntarily.
The force generated by a reflex cough can reach 100 miles/hr. The voluntary cough can vary greatly from just a short repeated cough commonly called a nervous cough to a forceful cough with the use of all muscles including accessory muscles of inspiration as in cases of bringing up thick tenacious sputum. When a cough brings up blood - is called Hemoptysis.
Factors triggering coughs.
Irritants: Irritation of the pharynx, trachea-bronchus from irritant gas, or fine sprays of chemicals like perfume, incense, household cleaners, and detergents.
Infectious agents: respiratory viruses, Covid-19, influenza, bacterial, fungal, mycobacteria.
Allergy and asthma.
Sinus and nasal discharge: Postnasal drip and vasomotor rhinitis, allergic rhinitis are some examples.
Medication: ACE inhibitors.
Pulmonary fibrosis: Idiopathic pulmonary fibrosis, post viral pneumonia fibrosis. Rheumatoid arthritis, SLE and scleroderma.
Malignant lesions: larynx, vocal cord, and Lung.
Aspiration of gastric acid: gastric reflux and aspiration.
Foreign body in airways.
Anxiety and psychosocial: also called nervous cough.
Putting a Q-tip in the ear.
Voluntarily or on request by the examining physician.
Types of Coughs:
Wet cough. In infection and allergy, where a lot of nasal secretion is generated.
Dry cough. Commonly seen in the use of ACE inhibitors, Pulmonary fibrosis.
The patients cough repeatedly, a short unproductive cough, involuntarily, and at times disturbs sleep.
Paroxysmal cough. The patient coughs uncontrollably and violently followed by a whooping sound in an attempt to resume breathing. Patients soon feel exhausted from coughing as seen in whooping cough(pertussis)
Tickle cough. In vasomotor rhinitis and allergic rhinitis, sudden onset of cough occurs and continues till secretions are completely cleared from the airway.
Nervous cough: repeated attempts to clear the throat when there is no secretion.
Croup. This is seen in children under 5 yrs. old in viral infection because of narrow airways. The swelling in and around the larynx produces raspy and squawking sounds.
Persistent cough. When cough persists over 6-8 weeks, as often seen in allergy and gastric acid aspiration. In delayed diagnosis like eosinophilic bronchitis, carcinoma of the lung, TB, fungal infection, etc.
Night cough. It is usually seen in gastric reflux and asthma.
Features of vasomotor rhinitis:
The precise cause is unknown, various agents are suspected including weather, perfumes, alcohol and spicy food. The cough follows a sudden gush of nasal watery discharge. The disincentive signs are the absence of an itchy nose, watery eyes, or scratchy throat.
Complications of persistent cough:
Most coughs are episodic, related to the upper respiratory tract infection, and are controlled easily. In prolonged vigorous cough, some of the following complications may be seen.
Fainting spells, Subconjunctival hemorrhage, small urine leaks, Inguinal and femoral hernias, Fractured ribs, Sore chest wall and costochondritis. Exhaustion, Sleep deprivation.
*****************************
No comments:
Post a Comment