Nasal Septum
PKGhatak, MD
Humans have one nose but two nasal openings called nasal passages. The two passages are separated by a central partition, made up of bony plates and one piece of cartilage. The diagram below shows pieces of bone and one cartilage forming a vertical nasal septum.
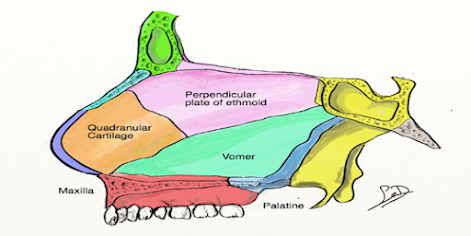
1. perpendicular plate of ethmoid bone (pink)
2. vomer bone. (green)
3. cartilage of the septum (khaki).
4. crest of the maxillary bone. (brown)
5. crest of the palatine bone. (blue)
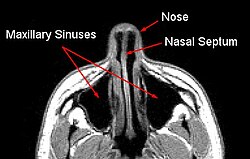
A CT scan view of the nasal cavity and nasal septum.
How the nasal septum developed:
In the early embryonic stage of development, two nose buds (nasal placode) develop from the neural crest. Evolutionary embryology documented how the human nose transformed from an olfactory organ to dual functions of respiration and olfaction through various stages of transformations. In the end, several facial and skull bones participate to form the nose and the nasal septum. The cartilages fill in places where injuries and deformities are likely to take place.
Nostril in other animals.
Sperm whales, dolphins, beluga whales and orcas have one nostril, also called the blowhole, the second nostril is modified as an echolocation organ.
Fish use gills for respiration and have 2 to 4 nostrils. One set is used to take in water to a chamber for detection of odor and the other two to discharge water.
Octopuses, crabs and butterflies have no nostrils. Snakes have no nostrils, an opening of the airway called the gullet is located just behind the tongue and is kept closed until the snake swallows air, then directs air to its lungs. Snakes can protrude the gullet to one side of the mouth while swallowing a large prey and at the same time breathe. The snake collects odor molecules from the air by flicking out its tongue repeatedly and when the tongue is retracted into the mouth, a special organ located on the palate generates the sense of smell.
Variation of size and shape of the nasal septum.
It is said that people in hot and humid tropical areas have flat, wide noses and a flatter nasal septum because for a given amount of air, the oxygen content is lower than what is present in a cold climate. As a result, a larger amount of air is necessary and a wide short nose is more suitable for such a purpose. In a cold climate, the air has to be warmed up to body temperature quickly. A higher nasal bridge and a larger nasal septum increase the surface area and warm up the air in a shorter time.
Embryology:
Nasal septum development is a part of the development of the face. It is difficult to summarize its embryology in a few short sentences. The link below can be used to access a more detailed description.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7965203/figure/F4/
[Also see the footnote].
Head ectoderm, neural crest and prechordal plate by repeated fusion and separation from a common oral-nasal cavity. The midbrain neural crest migrates below the nasal placode (a plate like thickened epithelial layer) and develops as the lateral nasal process and the forebrain neural crest forms the medial nasal process. As these cavities begin to deepen, a middle ridge appears. This medial ridge develops as the vertical plate of the maxillary bone. Other bones and cartilage follow the same pattern and ultimately a nasal septum comes into shape.
Histology of Nasal Septum.

The nasal septum is about 2 mm thick. Both surfaces of the nasal septum are covered by mucous membrane and the submucous tissue contains blood vessels and nerve tissue. The surface of the mucus membrane is covered by epithelial cells, which have 3 different forms. See the diagram below.

At the front end of the septum, the surface is covered by keratinized stratified squamous epithelium. The major portion of the septum is covered by respiratory epithelium which is the pseudo-stratified columnar ciliated epithelium. The uppermost part, below the cribriform plate, is covered by olfactory epithelium. These cells are tall columnar cells and support the olfactory cells.
Olfactory epithelium.
The olfactory epithelium contains Odor sensing neuronal cells and supporting cells, basal cells and brush cells.
Olfactory cells. These are bipolar cells, the top part facing the nasal cavity is supplied by hair cells (modified cilia). Its function is to trap odor molecules, helped by watery secretion from glands in the submucosa. From the base of the bipolar cells, the nerve fibrils emerge and the nerve fibers pass through the cribriform plate and make synaptic connections with the Mitral cells of the olfactory bulb.
Supporting cells. These are pseudo-stratified ciliated columnar cells. Functionally, cells are of two types. The sustentacular cells and microvillar cells. The sustentacular cell metabolically supports the respiratory epithelium. Microvillar cells are endowed with immune functions.
Basal cells divide actively and transform into other cell types, including bipolar nerve cells.
Brush cells. They are columnar cells and have microvilli. Brush cells are general somatic sensory receptor cells of the trigeminal nerve branch of the nose.
Cavernous tissue. Erectile tissue covers the turbinate (overhanging structures of the lateral wall of the nasal cavity), it is also present at the junction of bone with the cartilage. The blood in the cavernous tissues quickly warms air when the artery is dilated by parasympathetic signals.
Blood supply to Nasal Septum.
The nasal septum has a rich blood supply and several arterial branches of both the internal and external carotid arteries, which join together into an arterial plexus. From this plexus, the septum receives its arterial supply. The anterior inferior part of the vestibule (the place people put their fingertips) is known as Little's area and is the main area of the source of nose bleeds. The four arterial branches that join together to form the Kieselbach plexus are - the Sphenopalatine artery, a branch of the internal maxillary artery, which is a branch of the external carotid. The anterior ethmoidal artery, which is a branch of the ophthalmic artery, originates at the circle of Willis, comes from branches of the internal carotid artery. Septal branches of the superior labial artery, a branch of the facial artery. Posterior ethmoidal artery, a branch of the maxillary artery.

Venous drainage.
A submucosal venous plexus drains blood to the Sphenopalatine vein and ophthalmic vein. These veins make a connection with the cavernous sinus of the brain (a potential source of brain infection).
Nerve supply to Nasal Septum. The origin of the Olfactory nerve is stated earlier. The general somatic sensation (pain, pressure, heat & cold) is supplied by the sensory division of the 5th cranial nerve. The ophthalmology branch of the 5th cranial nerve supplies the upper anterior of the septum, the maxillary division of the 5th supplies the posterior and inferior part of the septum.
Parasympathetic secretory innervation of nasal glands originates in the parasympathetic nucleus of the 7th nerve, the preganglionic fibers synapse in the pterygopalatine ganglion and postganglionic fibers innervate the nasal glands. Stimulation of this nerve dilates blood vessels and increases nasal secretion.
The sympathetic nucleus is present in the Thoracic 1st segment of the spinal cord, preganglionic fibers travel up and make a synaptic connection in the Caudal sympathetic ganglion. Postganglionic fibers travel along blood vessels to reach the nasal glands, Stimulation of this division produces vasoconstriction and relieves congestion.
Lymph drainage of the nasal septum to the posterior deep cervical and submandibular lymph nodes.
Structural abnormalities of the nasal septum.
A common deformity comes from a direct injury to the nose resulting in a fracture of the bones of the septum but the cartilage withstands many less severe blows because of its flexibility and side to side mobility. Both congenital and acquired diseases can alter the shape and character of the septum.
Genetic abnormality.
Cleidocranial dystocia is an autosomal dominant trait. It is characterized by short stature, sloping shoulders, absent collar bones and deformed nasal septum.
Down syndrome babies have saddle shaped nose, a short neck, a protruding tongue, and exhibit mental developmental delays.
Congenital.
Congenital syphilis produces destruction of nasal cartilage and a saddle nose, frontal bossing, saber shins and many other abnormalities.
Acquired condition.
Relapsing Polychondritis.
It is an autoimmune disease that develops around midlife. Inflammatory destruction of respiratory cartilages, a saddle nose is the common finding.
Cocaine abuse. Cocaine snorting produces ischemia and as a result perforation of the nasal septum develops. Cocaine use causes frequent sinus infections.
Leprosy. Untreated leprosy can destroy cartilage and bones of the face and nose, and many other systemic symptoms.
Leishmaniasis. Mucocutaneous sores may erode nasal bones and soft tissue and other areas of the mouth and face, leading to many secondary infections.
-------------------------------------------------------------------------------------------
Footnote: -
Root. The uppermost portion of the nose is just below the eyebrows.
Bridge. The part that connects the root to the rest of the nose.
Apex. The tip of the nose.
Nostril. The opening of the nose is also called naris (pleural – nares).
Ala. The side wall of the nostril (pleural – alae).
Philtrum. The part connecting the tip of the nose to the upper lip. It is concave in shape.
**************************************