Eardrum
PKGhatak, MD
The eardrum is known as the Tympanic membrane (TM). The word Tympanum is a Greek word, it means to beat or strike. The Latin of the eardrum is Myringa and inflammation of the tympanic membrane is known as Myringitis.
The eardrum is about 1 cm in diameter, located at the end of the ear canal, positioned in a slant fashion, with the external surface facing downwards and forward, looking towards the face.
Structure. It is made of three layers. The outer surface. The middle fibrous portion and the inner surface.
A thin layer of skin tissue covers the outer surface, these cells are stratified squamous keratinized epithelial cells. The middle layer is a tough connective tissue made up mostly of type II and type III collagen and this layer contains blood vessels and nerve fibers. The inner surface is made of cuboidal epithelial cells, which are continuous with the lying cells of the middle ear.
Embryology.
In a developing embryo, an invagination of the first pharyngeal groove joins the first pharyngeal pouch. These two layers form the TM. The outer layer is Ectodermal in origin and the inner layer is derived from the Enteroderm. The middle layer is derived from the neural crest, a mesenchyme tissue.
Blood Supply. The TM has two different blood supplies. The blood supply of the outer surface is provided by the deep auricular branch of the Maxillary artery. The inner surface is supplied by the anterior auricular artery, which is a branch of the maxillary artery. The posterior part of the inner surface is supplied by the posterior tympanic artery, a branch of the posterior auricular artery.
Nerve supply. The inner and outer surface of the TM is supplied by separate nerves.
The sensory supply of the outer surface. The cranial nerves – the 3rd (Trigeminal), the 7th (Facial), the 10th (Vagus) and the 11th (Glossopharyngeal) supply different areas of the outer surface. The inner surface is supplied by the cranial nerve 11th.
Attachment of TM to the bones.
The outer rim of the TM is thick and cartilaginous. That fits snugly with a groove of the mastoid bone; however, the ring is not complete, a segment of the top is devoid of the ring, as a result, this part is less taught and called pars flaccida.
Bone attachment to TM:
In the middle of the inner surface of TM, the manubrium of the Malleus bone is attached. It pulls the TM inwards and gives it a conical shape; the inner side takes a convex shape and the outer side assumes a concave appearance.
When the TM is observed under direct vision with a scope, the different areas are identified with specific names; a diagram is easier to point this out.

The Tympanic membrane
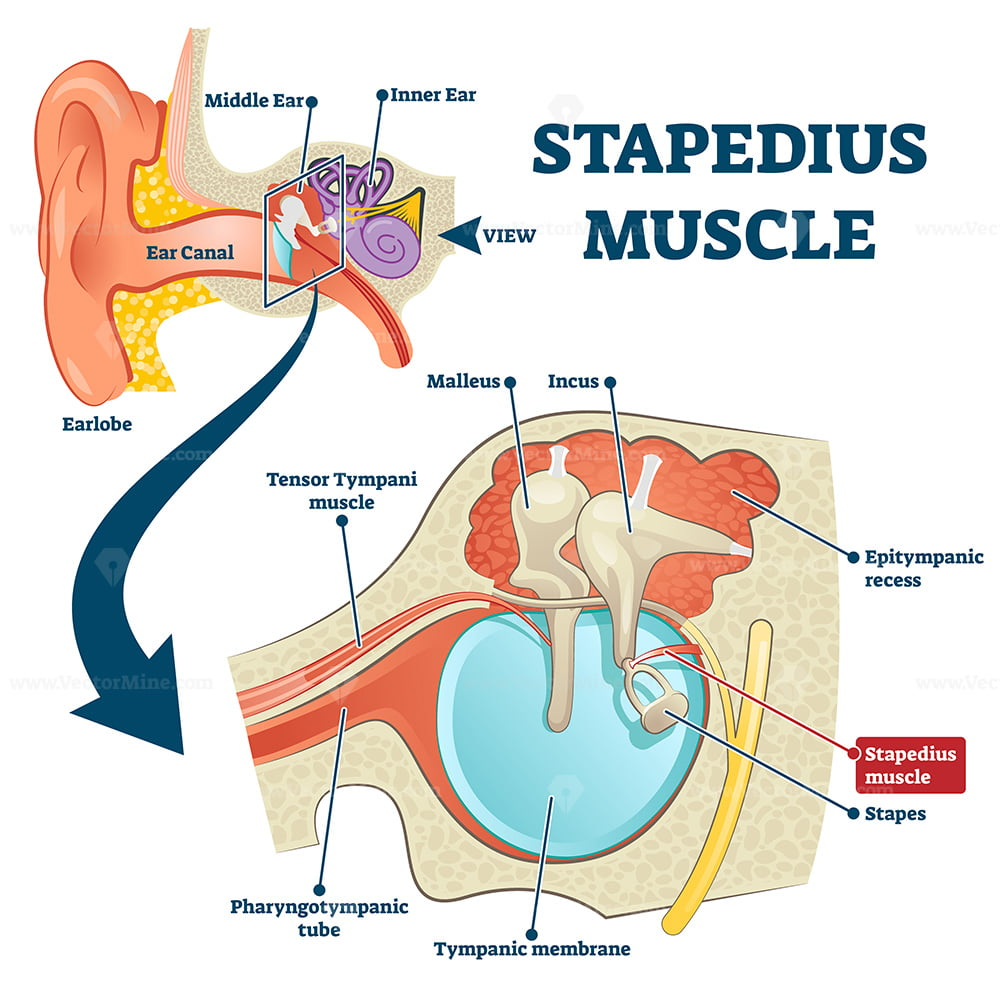
Protective muscle of the middle ear.
Two small muscles, the tensor tympani, and stapedius muscles protect delicate hearing organs by reflex action. The motor fiber for the Tensor tympani comes from the Trigeminal nerve (motor division) and the Stapedius muscle is supplied by a branch of the facial nerve. Tensor tympani by contracting increases the tension of TM and reduces the amplitude of vibration. Stapedius can disengage the stapedius bone from the oval window of the inner ear in order to protect the delicate sound receptors and the hair cells.
Function of TM.
TM is a physical barrier between the middle ear and the ear canal. It prevents water, dirt, dust, small insects, etc. from getting inside the middle ear.
TM transmits sound waves to the 3 small bones directly, the bones in turn transmit the sound waves to an opening of the bony Cochlea, the Oval window and the sound is transferred to the endolymph of the membranous cochlea and thereby to the hair cells.
The surface area of TM is 64.3 mm square. The surface area of the Oval window is 1/120 of the surface area of TM. The sound waves are magnified 27 times by the time it reaches the endolymph of the cochlea.
Diseases of TM.
In adults, diseases of TM are not common. Injuries usually result from blast injuries in certain professions using dynamite and in warfare. Inflammation or infection from the ear canal can spread to the TM. Such infections usually develop in swimmers, due to moisture-loving bacteria like Pseudomonas or Atypical tubercular bacteria.
In children, TM injury or infection is common. Injuries result from improper use of Q-tips. Throat infections rather easily spread to the middle ear and then to the TM because the Eustachian tube in children is short and does not drain so easily as in adults.
A few special diseases of TM.
Bullous Myringitis.
Bacteria, Mycoplasma and Virus infections occasionally produce not only acute infection of the TM but also produce a fluid filled blister on the TM. Blisters may be hemorrhagic. This was found to be common in Mycoplasma infection, subsequently, bullous lesions are also observed in bacterial and viral infections. Myringitis is a painful febrile illness, that often results in perforation of the TM and a temporary decrease in hearing.
Swimmer's ear itches.
Cotton from the Q-tip gets dislodged in the ear canal, which blocks the drainage path. Stagnant water favors Pseudomonas aeruginosa and Staphylococcus aureus growth. Acute infection later becomes a chronic spreading infection from the TM to the entire external ear.
Swimming pool granuloma. Mycobacterium marinum can cause a chronic ear canal and TM infection, usually from minor wound infection. It produces granulation tissues and damages ear canal, if not properly treated.
Ramsey Hans Syndrome. It is an uncommon illness characterized by paralysis of one side of the face and the appearance of a bunch of blisters, including on the TM due to reactivation of the chicken pox virus, often called shingles. Pain in the ear, loss of hearing on the side of facial paralysis and difficulty in speech and in attemting to eat food collects betwen the lip and gum.
Cholesteatoma of the ear.
Retracted TM or perforated TM if left untreated for a long time, causes accumulation of dead skin in the inner side of TM and in the middle ear. Occasionally skin grows into a lump or cysts develop. The accumulated wax starts to eat away the bone and recurrent infections lead to the formation of osteomyelitis in the mastoid bone. Fowl smelling discharge, loss of hearing, sensation of fullness of ear and dizziness develop.
Rupture and perforation of TM.
Ruptures are mostly accidental due to a sudden blast of air hitting the eardrum in milliseconds before the protective reflex action of the stapedius muscle can disengage from the Oval window.
Barotrauma. Air pressure of both sides of the TM is equal due to a reflex action of swallowing, yawning or clearing the throat. In a sudden change of air pressure, like an airplane taking a nose dive or loss of cabin pressure and many other situations, the decreased ear canal pressure causes TM to bulge out so suddenly that it actually ruptures.
Perforation of TM. Acute otitis media with large effusion or pus formation in the middle ear pushes the TM outward, and treatment is delayed, the TM ruptures and drains pus outside. Other causes of TM perforations are instrumentation, attempts to clean wax using unorthodox methods. Severe head trauma. Deep water diving or Caisson's disease.
Deliberate act. Bajau people of the Philippines, Indonesia, Malaysia, engaged in deep water hunting, used to deliberately puncture their ear drums so to prevent accidental rupture during deep dive, and miss to earn a living wage for a few weeks.
Retracted ear drums. Retraction of TM is a common occurrence, in most cases pars flaccida is retracted and nearly all resolve spontaneously. Only a few instances, the whole TM is retracted and due primarily to pharyngotympanic tube blockage. It is one of the causes of cholesteatoma.
Cancer of TM:
Cancer of the ear drum is very rare, however, the following cancers are possible: Basal cell carcinoma, Squamous cell carcinoma, and Melanoma.
The inner surface is the same as the lining membrane of the middle ear, if cancer develops, adenocystic carcinoma and adenocarcinoma are likely.
edited: January 2026
************************************************

No comments:
Post a Comment