Syndrome in Clinical Medicine
P.K.Ghatak,MD
ghatak3@gmail.com
In
a NIH publication in 2003, Dr. Franz Calvo et al, defined syndrome as
a recognizable complex of symptoms and physical findings for which a
direct cause is not necessarily understood. Once the medical science
identifies a causative agent or process with a high degree of
certainty, physicians may then refer the process as a disease and not
a syndrome.
Some
well known syndromes are now called diseases and to illustrate, an
example is Cushing's disease and Cushing's syndrome. In 1912, Dr.
Cushing reported a new disease he called polyglandular syndrome due to
malfunction of the Anterior Pituitary gland. He published this entity
in 1932 as basophil adenomas of the Pituitary body and named it
Pituitary basophilism. Symptoms of the disease - gained excessive
weight, mostly around the back of the neck, face and abdomen. Also
developed high blood pressure, diabetes, acne and facial hair. In
subsequent years, the condition was known as Cushing's syndrome.
Further studies identified
the cause was a tumor of the anterior pituitary producing an excess
amount of ACTH hormone, which in turn put out excess
corticosteroids from the Suprarenal glands. Similar changes were also
detected when patients took steroids for a prolonged time, as one of the
anti-rejection drugs following kidney transplants. And also seen in
certain cancers of the lungs secreting an excess amount of polypeptide
having similar hormone like actions of the suprarenal gland. Now
Cushing's Disease term is reserved for symptom complex arising from
tumor of the anterior pituitary and Cushing's syndrome is applied to all
other causes which can produce some features of Cushing's disease.
If
one looks up Syndrome in the Wikipedia, one will be surprised to find
more than 1600 syndromes. In the index of any textbook of medicine, where every entry is listed in alphabetical order, one finds only 3
entries under syndrome, the rest of the syndromes are under the first
letter of a name attached to the person who discovered the illness. Not
all the listed syndromes, however, follow this rule. Some names are
retained because the name refers to well understood symptoms by the
public, like - Milk - Alkali syndrome and Irritable Bowel Syndrome.
Recent
rapid advances in genetics, MRI imaging, sonography, immunology
and biochemistry have solved many obscure causes of syndromes. In the
lifetime experience of any well rounded physician, they might have not seen
more than 30 syndromes. Certain specialties like Pediatrics are likely to see more syndromes.
A
few syndromes will be presented, one or two from each group, to give the readers a chance to the readers the mystery about the syndrome.
Down
syndrome.
Down
syndrome arises from abnormalities of chromosome 21. It occurs in
75% of cases as inherited and 25% as spontaneous. Each cell of the body
contains an additional one full or partial copy of chromosome 21. This
generally happens as non-splitting or translocation between
chromosome 21 and 14 or 21 and 21 or 21 and 22. In 2 to 3 % cases it
also occurs due to Mosaicism.
Some
of the common features of Down syndromes are mental retardation, flat
cranium and flat nose bridge, a short neck, large tongue compared
with the floor of the mouth, prominent epicanthal fold, structural
heart defects, truncal obesity, poor muscle tone an delayed mile
stones of development.
Polycystic
Ovary Syndrome.
Originally, the Polycystic Ovary syndrome was called Stein-Leventhal syndrome
because this pair of investigators were the first to report it in
1935. In 1990, NIH added two additional criteria - multifactorial
genetic errors and insulin resistance, and finally in 2003, ultrasonographic detection of more than 20 cysts in the ovary was added and
named it Polycystic ovary syndrome. The cause of this syndrome is
unknown and symptoms vary widely.
A
typical case has these features: Symptoms of irregular and scant
menstrual flow or delayed menarche. Development of acne and facial
and body hair of masculine type, obesity, hypertension and insulin
resistance and diabetes mellitus. Most cases are due to excessive
androgen activities, but androgen is normal in the minority of cases. In a few cases, the polycystic ovary syndrome is detected during
investigation of failure to conceive. If not treated properly, there
is a high likelihood of development of endometrial carcinoma later in
life.
Klinefelter
syndrome. This congenital condition affects only male children due to
having an extra X chromosome. The condition is also known as 47 XXX.
The genetic abnormality occurs randomly either in the development of the ovum or sperm. The condition is generally detected at puberty when
the child failed to develop muscle mass and develop a feminine body
type - gynecomastia, no facial hair and wide hips. They have small
genitalia and testicles, scant or absent sperm production and have
long legs and a short torso. Many have learning difficulties and lag
behind in reading and writing skills.
Not
all affected have all the above features and may pass as normal and
only correctly diagnosed much later when one fails to father
children. They carry the risk of breast and extragonadal germ cell
cancers and also osteoporosis.
Turner's syndrome. Turner's syndrome is also known as 46 XO. This congenital condition is seen only in female offspring, arises due to missing a whole or part of the sex chromosome X; but whether that missing X chromosome is paternal or maternal is not known. The gene responsible for bone growth is the SHOX gene and it is missing in Turner's syndrome, resulting in the abnormalities of bones in Turner's syndrome. At birth the child may appear normal except for a web neck and a broad chest. As the child reaches age 9 or 10, the growth slows down, develops no secondary sexual characters and menstrual cycles. Other features are cubits vulgus, aortic/ pulmonary stenosis and high BP, diabetes mellitus, hypothyroidism and osteoporosis.
Fragile
X syndrome: It is a X link cause of mental retardation. Males are more
severely affected than females. Incidence is 1:4000 male births and
1:10,000 in females. Symptoms in female are learning difficulties,
variable degrees mental retardation and early onset of menopause. In
males, the physical characteristics are large ears, a prominent jaw bone,
a pitched voice, Mitral valve prolapse and increased immobility
of joints. This syndrome is associated with autism.
The
tip of the long arm of chromosome X carries the mutated Fragile RNA gene, results from undue expansion of CCG repeats. More repeats are present
more mental retardation is detected.
Marfan
syndrome. Marfan syndrome is an autosomal dominant inherited disorder
of the connective tissue due to mutations in the Fibrillin gene
(FBNA1) on chromosome 15. This results in aberrant TGFB1 and TGFB2
activities. Clinical features of Marfan syndrome are tall stature,
long arms and legs, scoliosis, pigeon chest wall deformity(Pectus
excavatum), dislocated eye lenses, mitral valve prolapse, aortic root
dilatation, aortic incompetence and aortic aneurysm and dissection.
Ehlers-Danlos
syndrome. This is another connective tissue autosomal dominant
inherited disorder. Mutation of many genes, the last count 20 genes, are
implicated, and based on the severity of symptoms, 11 varieties are known.
Those who have severe symptoms have a mutation of COL5A1 and COL5A2
genes, other mutated genes are TNXB, ADMTS2, PLOD1, FKBP14 and many
others. Mutations result in the formation of collagen tissue in a
haphazard fashion and functionally of poor quality specially of the
skin, skeletal muscles, arteries, bones and internal organs. Major
symptoms include fragile velvety skin, which peels off easily and
forms extensive scars. Aneurysm of the artery and dissection and rupture
of aneurysm and other changes of the eyes, heart and bones mentioned
under Marfan syndrome.
Irritable
bowel syndrome. Irritable bowel syndrome fits the classical
definition of the syndrome. A group of symptoms originates in the colon
and small intestine but the cause remains unknown. Common symptoms are - a
sense of not being able to evacuate completely after a bowel movement,
constipation and low grade abdominal cramps, flatulence and diarrhea,
often hard and lumpy stool and diarrhea on the same day, and several
bowel movements a day. Various theories are put forward, including
stress, pressure of modern life, precooked meals, food additives,
change of colon bacterial colonies and low tolerance to pain. Both
sexes are affected and the age of onset - from teens to elderly. It is a
common illness.
Milk-Alkali
syndrome. It is a self made syndrome due to taking an excessive
amount of Calcium supplement to prevent osteoporosis and the condition is
accelerated and made worse by taking a mega dose of vitamin D3. In the previous
generation, people suffered this complication from taking excessive
amounts of Tums, Maalox and Mylanta for heartburn and peptic ulcer
diseases. Excess alkali present in the form of carbonate in these
compounds shifts the blood pH towards the alkaline side. High blood
calcium results in an excess amount of calcium excreted in the urine.
Kidney stones and urinary bladder stones may develop. Renal colic,
chronic pain around the loin and back are usual symptoms of kidney stones.
Left untreated, patients may end in renal failure.
Abdominal
Compartment syndrome. This is a serious and often fatal condition that arises from several causes but is often seen in severe burn victims.
Other causes are organ transplants, prolonged abdominal surgery
specially repair of abdominal aorta rupture, bullet or knife
penetrating injury with severe intra-abdominal hemorrhage. Sepsis,
abdominal abscess, severe peritonitis and others. Fluids and
inflammatory exudates accumulate in and around organs and raise
intra abdominal pressure over 20 cm of Hg. This impairs arterial
supply and blocks venous and lymph drainage, producing further damage to the abdominal organs. Immediate proper fluid management and abdominal
surgery is needed to relieve the high intra abdominal pressure.
Sudden
Infant Death Syndrome (SIDS). A healthy newborn child suddenly stops
breathing and dies during sleep. In the majority of cases are due to
suffocation due to putting children face down in a soft bed for
sleep; which favors obstruction of the mouth and nose. About 20 % of cases remain unknown.
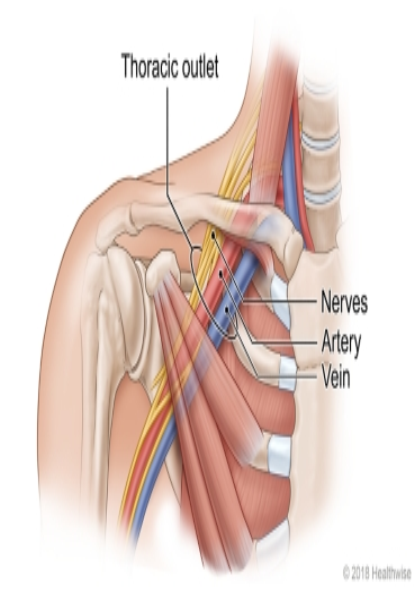
Thoracic
outlet syndrome.
Just below the clavicle at a point it turns towards the shoulder, the Subclavian artery the subclavian veins and all the nerves arise from the brachial plexus, enter the chest wall and course down the medial side of the arm. There is just enough room for the structure to pass. In an abnormal situation like fracture of the clavicle and hematoma formation, a cervical rib and osteoma of the first rib that space becomes too tight for these structures and pressure on artery produce pain in the arm and hand, pressure on the vein swelling of hand and forearm and bluish discoloration of fingers, Pain over the nerve produces tingling numbness of fingers and muscle weakness. The pressure must be relieved by surgery to prevent permanent damages to the hand.
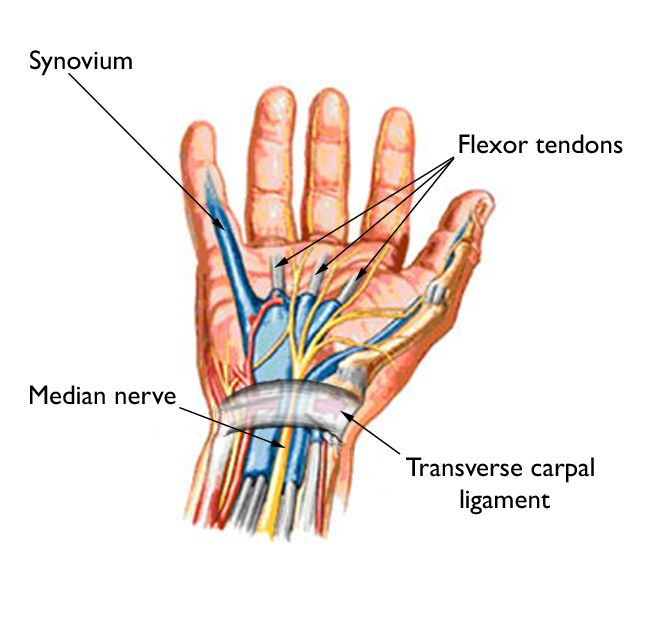
Carpal
tunnel syndrome.
This is another syndrome like the thoracic outlet
syndrome due to anatomical peculiarity at the flexor surface of the
wrist. The median nerve on the way into the palm of the hand has to
negotiate through a narrow passage in between wrist bones- Pisiform
laterally and Hamate and Capitate inferiorly and a strong transverse
carpal ligament anteriorly. Pain, specially at night, numbness and
tingling are the initial symptoms felt in the hand and fingers, at
times the pain is felt in the forearm. Later weakness of fingers and
thumb, muscle atrophy and ultimately claw hand develops. The causes
of Carpal tunnel syndrome are several - Unaccustomed weight bearing, repeated flexion and extension of the wrist, pregnancy, fracture of
wrist bones and malunion of fractures, synovitis of the flexor
tendons, hypothyroidism and myxedema, rheumatoid arthritis,
amyloidosis, sarcoidosis, acromegaly and leukemias.
Tarsal
tunnel syndrome. Just like carpal tunnel syndrome, Tarsal tunnel
syndrome may develop at the ankle joint. Symptoms and causes are
practically the same except for the site.
Inappropriate
ADH secretion. Blood volume and serum osmolarity are maintained by
feedback loops on the control center located in the hypothalamus and
posterior pituitary gland. In lower blood sodium concentration and excess water content of blood (low osmolarity), no Anti Diuretic Hormone (ADH)
should be released from the posterior pituitary. But if ADH is still
released in such a condition, the situation is called Inappropriate ADH
secretion. The causes are many, however, Lung cancer, encephalitis, meningitis, subdural hematoma are main causes.
Syndrome
X. Syndrome X is due to abnormal microcirculation of the coronary
arteries or coronary vasospasm, which results in Angina pectoris.
Syndrome
of apparent mineralocorticoid excess, This syndrome is due to 11 beta
hydroxysteroid dehydrogenase deficiency inherited on an autosomal
recessive mode. Symptoms are early onset of hypertension in
childhood, low serum potassium and metabolic alkalosis.
Metabolic
syndrome. Metabolic syndrome is a more recent entry in the syndrome
category; previously the components of this syndrome were known as
essential hypertension, hypercholesterolemia, obesity and diabetes
mellitus. Under the new name, those previous entities are refined and
redefined, instead of hypercholesterolemia, it is now low HDL
cholesterol and high triglyceride. Obesity is now abdominal obesity,
Diabetes is replaced by above impaired fasting blood glucose.
People with Metabolic syndrome are at high risk of developing coronary
arterial disease, diabetes mellitus and cerebrovascular accidents.
Stokes
- Adam syndrome. This syndrome was well established a century ago,
when physicians used their well cultivated skill of observation and
taking pulse over several minutes. Main features of Stokes-Adam
syndrome are sudden loss of consciousness, and fall to the ground and
having epileptic seizures due to complete heart block ( third degree
in new definition) and a pulse rate of 35 or below. Ventricular
fibrillation and ventricular tachycardia also unconsciousness and
seizures. At one time it was called Cardiac seizure and that name
was better known than Stokes-Adam syndrome.
Long
Q-T syndrome. This is an electrocardiogram finding. The time interval
between the beginning of the q wave and the end of the T wave on the tracing of
an ECG (EKG) is normally 0.43 millisecond when the heart rate is 72/
minute. In a slower heart rate, the Q-T interval increases predictably. In several cardiac diseases and quinine, procainamide, digitalis,
over-the-counter cold medicines and many other medications can cause
undue prolongation of Q-T interval. The longer the interval, the greater chance there is of Ventricular ectopic beats and precipitation of
ventricular tachycardia and ventricular fibrillation. A particular
form of multifocal and multidirectional ectopic ventricular
beats called Torsades des pointes (a French word, meaning twisting
around points) is a forerunner of Ventricular fibrillation and death.
Torsades des pointes
Sick
sinus syndrome. This is another very significant ECG finding. The
natural cardiac pacemaker is the sinus node. In oxygen deprivation
from any reason, electrolyte imbalance and certain medications, the sinus node fails
to generate the electrical pulse wave for the heart muscle to contract.
This can manifest as slow heart rate over 3 seconds, 1st,
2nd,
and 3rd
degree heart block. These changes are variable and in some cases variable cardiac block can be
intermittent. To detect the condition, a special cardiac monitor is
used, which can trace every cardiac beat and record on a preset
program. This allows closer examination of any abnormal heart beat and suitable treatment can be offered – often a
pacemaker. Main symptom of sick sinus syndrome is missing a heart
beat, irregular pulse, palpitation, fluttering sensation in
chest, confusion and loss of balance and fall.
Goodpasture
syndrome. Goodpasture syndrome is an example of how an antibody, generated
to fight an unidentifiable infection, mistakes its own kidneys as
foreign and attacks the collagen tissue present in the basement membrane
of glomeruli and walls of alveoli of lungs, results in
hemorrhage in the kidney and lungs. Main symptoms are bloody urine
and coughing out of blood. Other significant symptoms are shortness
of breath, chest pain, fatigue, anemia, high BP, fatigue, nausea
and vomiting. It is a major illness and requires immediate medical
attention.
Alport
syndrome. Alport syndrome is a multisystem inherited disorder involving
collagen IV tissue and results in renal failure, deafness and visual
impairment. The defective gene is carried on the X chromosome. Male
child develops glomerulonephritis at an early age and progresses
rapidly and unless treated, dies by age 40, females are less
frequently affected and the disease progresses slowly.
Nephrotic
syndrome. Nephrotic syndrome is a stage in renal failure that arises from
protein losing glomerulonephritis. Presence of a large amount of protein in the urine makes urine foamy, hypoalbuminemia produces puffy eyes, pale puffy face, ankle
edema and scrotal edema. With the further progression of disease, ascites
and plural effusion are seen. Anemia, fatigue, weight gain from accumulated water develop. Intercurrent infection is common.
Carcinoid
syndrome. In a previous blog, carcinoid syndrome was discussed in
detail. See footnote.
Carcinoid
syndrome is due to the production of many polypeptides which have hormone like effects released from one variety of neuroendocrine tumor. Carcinoid tumors generally arise in the small intestine, stomach, colon, appendix,
rectum and liver and pancreas, and also arise in the bronchial tree
of the lung. Carcinoid secretes serotonin, histamine, kallikrein,
tachykinins and prostaglandin. These are potent vasodilators and
produce intense vasodilatation, hypotension, watery diarrhea, asthma
like bronchospasm and intense flushing of the face and body. The
tumors are small and can be benign or malignant, but pathologically
can not be determined whether a tumor is benign or malignant. In malignant variety, the tumor metastasizes
in the liver.
Dumping
syndrome. Dumping syndrome is a number of gastrointestinal symptoms that occur a few minutes after a meal. Vagotomy and reducing stomach
capacity by surgery are the principal causes of Dumping syndrome.
Following any such stomach surgery, the food leaves the stomach
prematurely and enters the duodenum in large amounts overstretching
the duodenal wall, causing upper abdominal crampy pain, sense of
abdominal fullness, nausea, diarrhea, weakness and lightheadedness.
And later develops palpitation and rapid heart beats.
Short
bowel syndrome. Certain medical illnesses require taking out a part
of the small intestine. The small intestine becomes shorter. This
changes the absorptive capacity of the small intestine and patients
develop loss of weight and nutritional deficiency. Crohn's disease and
ischemic bowel are most common causes.
Zollinger-Ellison
syndrome (Z-E Syndrome). Z-E syndrome is due to Gastrin producing
tumor - Gastrinoma of the duodenum or pancreas. Gastrin stimulates
gastric acid production. The majority of Z-E syndrome cases are spontaneous in
origin but 25 % are due to Multiple endocrine neoplasm of type 1(MEN1). Several complications generally develop and are pretty serious –
gastric perforation and profuse Gastric bleeding, esophagitis and
esophageal atresia.
Budd
Chiari syndrome. This syndrome is due to hepatic vein thrombosis, which produces liver enlargement, upper abdominal pain, hepatic
necrosis, followed by centrilobular fibrosis and jaundice and liver
failure. Patients may develop this condition due to a hypercoagulable
state from inherited conditions like Factor V Leiden, Protein C and S
deficiency or from acquired conditions like myeloproliferative
disorders or Paroxysmal Nocturnal Hemoglobinuria.
Sjogren
syndrome. This syndrome is named after a Swedish physician, Dr
Henrik Sjögren, who reported cases of chronic arthritis associated
with dry eyes and dry mouth. It is an autoimmune disease producing
chronic lymphocytic inflammation of salivary and lacrimal glands.
The microvascular and ductal blockage results from inflammation, which produces dryness. In addition, exocrine glands of the skin, GI tract,
joints, lungs, CNS and kidneys are involved. Arthritis of the hand
resembles rheumatoid arthritis. ANA blood test is positive over 1:256
dilution and in addition SS-A, SS-B and RP serology are positive.
Sjögren's patients run a risk of B-cell lymphoma (non-Hodgkin
lymphoma) and antiphospholipid antibody production results in
vascular thrombosis.
Gillian
Barry syndrome. This is an example of an Autoimmune nervous system
disease. Antibodies attack the myelin sheath of the peripheral nerve and the damaged sheath eventually damages the core nerve fibers of axons.
Peripheral neuritis causes weakness of muscles of the limbs, muscles of
respiration and face. What triggers antibody production is not known
but a viral infection is likely. From the onset of symptoms of muscle
weakness and tingling, numbness and pain, the disability reaches its maximum in 3 weeks, and respiratory failure develops.
Pickiwian
syndrome. Nearly 200 years ago, the Author Charles Dickens in his famous
publication “The posthumous papers of the Pickwick club”
described obese individuals who were awake but hypoventilate due to reduced
sensitivity to hypercapnia of the respiratory center and frequently
dozed off. Pickiwian syndrome is chosen to honor Dickens's astute
observation of human nature. People with this syndrome have a BMI over 30 kg/square M. Fat accumulates around the neck, chest, and upper abdomen, and have a blunt respiration drive even in the presence of the strongest stimulus, respiratory
acidosis and hypercapnia. Leptin insensitivity explaining the
reason for obesity.
Premenstrual
syndrome. Million of women suffers irritability, mood changes, weight
gain and puffiness of face and hands and feet before the menstrual
flow begins. These symptoms are due to hormonal changes necessary to induce shedding of extra growth of the endometrium, which developed in anticipation of
fertilization of an ovum and the beginning of pregnancy.
Congenital
Myasthenia syndrome. This syndrome is inherited by an autosomal
recessive pattern, and also rarely by an autosomal dominant mode.
Weakness of muscles of the eyelids, eye muscles that move the eyes,
muscles of chewing and swallowing are commonly affected. Repeated
movements make weakness worse. Mutation of CHRN gene is responsible
for over 50 % of cases, the rest of the cases are due to mutation of
RAPSN, CHT, COLQ, DBC7 genes. Children fails to suck breast milk. Swallowing and any normal physical activities are affected. Severity
of disabilities varies depending upon the mutated genes. All these
genes are responsible for providing the codes of protein synthesis required
for the normal functioning of the transmission of nerve signal across the
neuromuscular junction.
Eaton-Lambert
syndrome. Eaton-Lambert syndrome is an autoimmune disease. Immune
system produces antibodies which mistakenly attack the Calcium
Channels on the nerve endings. This results in fewer functional
pathways for nerves to deliver signals to the effector sites involving both somatic and autonomic nervous system. In contrast with Myasthenic
syndrome, repeated action improves muscle functioning. Small cell
carcinoma of the lung is the most commonly responsible for this
syndrome, other malignancies also can produce this syndrome. The leg
muscles are commonly affected; the effects of the autonomic nervous
system can be severe in the cardiovascular system and the urogenital system.
Wernicki
- Korsakoff syndrome. This syndrome is a combination of Wernicke
encephalopathy and Korsakoff psychosis. Chronic alcohol abuse is the
underlying cause of Vitamin B1 deficiency, which is the cause of this
syndrome; however, other nutritional deficiencies are associated. The
symptoms are - inability to develop memory of current events,
confabulation and talkativeness, lethargy, confusion and coma. MRI
shows atrophy of the thalamus, hippocampus, hypothalamus and enlarged
ventricles. The symptoms are reversible if treatment can be started
before Wernicki encephalopathy sets in.
Ramsey
Hunt syndrome. This is a special case of Shingles. The one side of the face develops palsy of lower motor neuron type and is associated with vesicular rashes
on the external auditory canal, pinna, mucous membrane of the oropharynx. This is due to reactivation of Varicella - zoster virus (chicken pox virus).
The symptoms are pain in the ear, deafness, tinnitus, vertigo,
balance and ambulatory difficulties.
Loeffler's
syndrome. Loeffler's syndrome is due to a very high eosinophil count in
the blood, associated with infiltrate of eosinophils in the lung
tissue producing pneumonia like symptoms and bronchospasm. In early days, it was due to ascaris lumbricoides parasitic infestation when
Ascaris larvae wandered around to find their final residing place in
the small intestine. The allergic reaction generated an eosinophilic immune reaction.
Now other parasites are known to produce similar reactions during
their tissue migration.
Waterhouse-Feldman syndrome. Waterhouse-Feldman syndrome is a real emergency
situation during a meningococcal meningitis with bilateral adrenal
hemorrhage due to toxemia. It produces acute adrenal insufficiency
manifested as shock, hypotension, vascular collapse and cerebral,
renal and pulmonary inefficiencies. Many other bacterial and viral
infections are also known to produce this syndrome. Immediate intervention to normalize
blood volume and tissue oxygenation must be instituted and
intravenous corticosteroids are administered along with antibiotics and
other therapeutic agents.
Gilbert
syndrome. This is an inherited benign liver condition involving
high blood unconjugated bilirubin level causing jaundice. Other
parameters of liver functions are all normal and no treatment is
required.
Osler-Weber-
Rendo syndrome. This is also known as Hereditary Hemorrhagic
Telangiectasia. This is inherited in an autosomal dominant mode. It is
due to the presence of multiple gene mutations. Arteriovenous
malformation is present on the skin, mainly on the face and mucous
membrane of the nose, mouth, stomach, GI tract, liver, lungs, spinal
cord and brain. Bleeding from involved organs can produce a wide
variety of symptoms, bleeding in the brain can be fatal.
Footnote: For further reading see https://humihealth.blogspot.com/Medical matters.
1. Carcinoid syndrome, - Carcinoid and Neuroendocrine tumors. Blog. Medical matters dated 13 June 2011. 2. Loeffler's syndrome. - Round worm Ascaris lumbricoides. Dec 6.2023 3. Korsakoff psychosis. - Speech disorder. Oct,16,202. 4. Sjögren syndrome. - Collagen & mixed connective Tissue diseases. Dcc14,2022. 5. Zollinger- Ellison syndrome. - Peptic ulcers. .Feb 16, 2023 .6. Polycystic Ovary syndrome. Insulin resistanceMarch10,2022. 7. Cushing's syndrome. Pituitary gland. August 20,2021. + Adrenal gland Oct22,2021. 8. Rumsey Hunt syndrome. Chicken pox Feb 16, 2023, 9. Myasthenic syndrome. Neuromusculat transmission, Dec22,2022. 10. Milk- Alkali syndrome. Kidney stones April 16, 2022.
revised; September 2025.
**********************************************************